Mohs’ Micrographic Surgery
Mohs’ Micrographic Surgery is a highly specialized method of removing and examining cancerous tissue to ensure its removal. Frederic Mohs first invented this procedure, which is named after him. For the most common forms of skin cancer (basal cell carcinoma and squamous cell carcinoma), this procedure has the highest cure rate (least chance of the skin cancer growing back).
- The area is cleansed with alcohol.
- The visible tumor is identified and marked (usually with a purple gentian violet marking pen)
- The area is numbed using tiny needles and injecting a local anesthetic
- The area is prepped (cleansed) using Betadine® or Hibiclens® to reduce the risk of infection.
- The tumor itself is often removed using a curette (small sharp tool) or cut out using a scalpel.
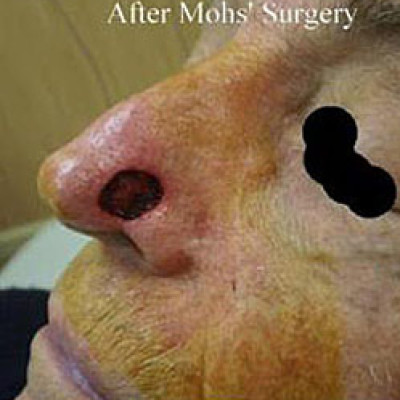
- A small margin (usually < 1mm) of normal appearing skin is removed all around and underneath the area where the tumor was. This is called Stage 1. This skin is used for examination.
- The skin removed from Step 6 is inked for orientation purposes so that if there is any cancer remaining, the surgeon can go to the exact location where it remains to remove more tissue (which would beStage 2, etc.).
- The tissue is then frozen and cut and placed onto glass slides that will be stained.
- The slides are then examined by the surgeon to ensure that all of the cancer is out. If the cancer is not all out, the surgeon can locate the area on the patient where cancer remains by the dyes that were used for orientation purposes and take an additional stage (see steps 7-9).
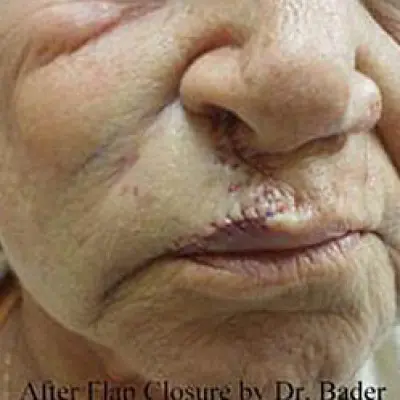
- After all of the cancer is out, the wound can be left to heal by itself (without stitches) or closed using stitches.
Common misconceptions about Mohs’ Micrographic Surgery:
1. “Mohs’ Micrographic Surgery leaves a big scar”.
False. Mohs’ Micrographic Surgery actually removes less normal (non-cancerous) tissue than nearly any other surgical modality and usually results in less scar. Mohs’ Surgery is a method used to remove tumors, it is not a method to repair the resultant defects. A bad outcome is usually due to one of the following reasons:
The defect (hole) after the tumor was removed was left to heal without stitches, when putting stitches in would have been a better option
The defect (hole) after the tumor was removed was closed with stitches, but the repair was not as good as it could have been.
The defect (hole) after the tumor was removed was closed with stitches, but the area did not heal well for one of many reasons.
The tumor was in a bad location or was a large tumor that resulted in significant scar.
Sometimes, additional surgery or other procedures may be needed to obtain an optimal cosmetic outcome.
2. “Mohs’ Micrographic Surgery costs too much money.”
False, in many cases. Several studies have shown that Mohs’ Micrographic Surgery is extremely cost-effective in the treatment of skin cancers in that it has the lowest recurrence rate (least chance of the cancer growing back). Mohs’ surgery is more costly than some treatments, but usually costs much less than radiation or surgery that is performed in a hospital or ambulatory surgery center. If you use two surgeons, i.e. one for Mohs and one for the reconstruction, the costs will be considerably higher. If your surgeon makes you come back on another day to have the reconstruction, it will cost more money and not in your best interest, but financially beneficial for the surgeon. Many surgeons take “too little” tissue, resulting in having to take more than one stage. This increases cost. A good and honest surgeon will try to get the tumor out on the first stage by removing the least amount of uninvolved tissue.
3. “Mohs’ Micrographic Surgery is not necessary.”
Many tumors do not require Mohs’ surgery and discussion with one’s doctor or Mohs’ Surgeon is recommended to help choose an appropriate treatment method. This procedure is often abused and overused, especially when one has the Mohs’ procedure performed in the same practice as the biopsy was done (i.e. when NOT referred out). Tumors on the nose, ear, lip, eyelids, genitals, and digits (fingers and toes) are commonly and often best treated with Mohs’ surgery. Tumors that are 1-cm or larger on the face are commonly treated with Mohs’. Large tumors that are 2-cm or great on the body can be treated with Mohs’ surgery. Some types of skin cancer are best treated with Mohs’, such as sclerotic or morpheaform Basal cell carcinoma.
4. “Mohs’ is inconvenient.”
The average wait time for slides to be processed and read in my office is 30 minutes. I believe that this is a small amount of time and is worth waiting for to ensure that all of the cancer is removed. Many offices have much longer wait times of an hour or more. This is not necessary unless the tumor is very large. Once a patient has clear margins, the closure is performed with minimal wait time. Other offices may have one have Mohs’ in the morning and wait until the afternoon to have the closure performed. Some offices will have patients come back on the following day, citing that “insurance only allows this”. This is untrue! Doctors get paid less to perform the closure and the Mohs’ on the same day, which saves money. Why would any patient want to have to come back the next day, waste time, and have to get re-numbed (which is not always comfortable) just so the doctor can make more money? Some patients are referred out to another surgeon to perform the reconstruction, which adds more cost and often more discomfort as the areas often have to be re-numbed. In short, most patients are in our office for Mohs’ and reconstruction for 90 minutes from beginning to end. That being said, some are here for hours for extensive cancers, which does happen every now and then.
About Robert S. Bader, M.D and his Mohs’ surgery training:
During his residency in Dermatology at MCP-Hahnemann University Hosptial, Dr. Bader had extensive training in Mohs’ Micrographic and reconstructive surgery. After residency, where he also served as Chief Resident, Dr. Bader completed a one-year fellowship in Mohs’ Micrographic Surgery and Dermatologic Plastic Surgery. Mohs’ Micrographic Surgery is only a method to remove a tumor. Following the removal of the tumor, Dr. Bader utilizes Plastic Surgery to recontruct the defect to leave the smallest possible scar. In fact, Dr. Bader is able to reconstruct 99% of the cases in the office immediately after Mohs’ Micrographic Surgery. In addition to the added convenience of having the procedure completed in one location on a single day in nearly all cases, one does not have to go to a hospital operating room or ambulatory surgery center, which can cost thousands of dollars.